1) Initial consultation
The process begins with an initial consultation with an orthodontist . During this phase, x-ray images, dental impressions, and facial photographs may be taken to assess the severity of the malocclusion. Once the need for orthognathic surgery is established, the patient is referred to a maxillofacial surgeon.
2) Simulation
A simulation can be performed to simulate the outcome and help the patient visualize the desired result. The before/after simulation also allows you to clearly explain to your surgeon what you want from the operation. Perform a simulation of a Class III skeletal surgery.
The maxillofacial surgeon will conduct a thorough evaluation, including clinical examinations, medical imaging, and a detailed analysis of the malocclusion. A precise surgical plan is developed to determine the necessary jaw movements.
3) Preparation for the intervention
Before surgery, the patient often undergoes preoperative orthodontic treatment to align the teeth and prepare the jaws for surgery. This involves wearing braces for several months or years.
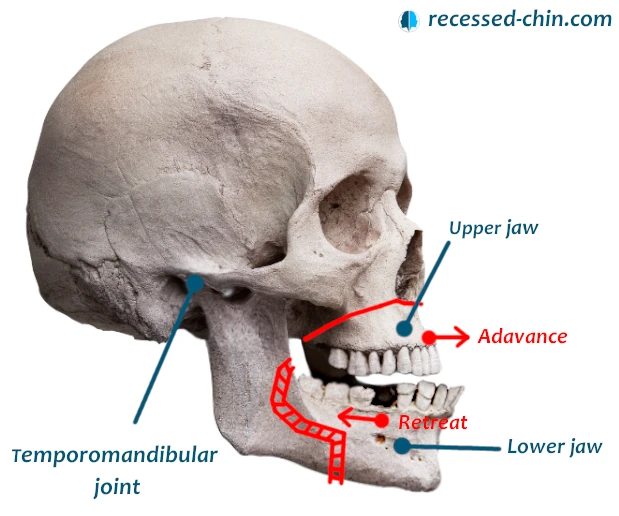
4) Day of intervention – Skeletal Class III
During surgery, the maxillofacial surgeon makes precise cuts in the jawbones to reposition them. The bones are secured with titanium screws and plates. They are biocompatible and do not beep at airports.
5) Post-operative period
After surgery, the patient is usually monitored for one day in the hospital. The length of hospitalization depends on the complexity of the procedure and the patient’s recovery: 1 to 3 days.
The patient then continues to recover at home, following the maxillofacial surgeon’s instructions. This involves a liquid or soft diet for a period of time and taking precautions to avoid stress on the recently operated jaws.
6) Follow-up
After the operation, the patient continues orthodontic treatment to adjust the position of the teeth and perfect the occlusion.